
Coronary Artery Disease is the most common acquired disease of modern era.
Depending on the severity of ischaemia, coronary artery disease it can present as-
- Chronic Stable Angina
- Chronic Unstable Angina
- Vasospastic Angina
- Myocardial Infarction
ECG is an important, easily available and reliable tool for diagnosing and planning treatment of a patient with CAD. However, clinical judgement other investigations are often required to confirm the diagnosis because ECG may not reflect the actual severity of ischaemia and underlying damage.
ECG can be normal in 1-6% of patients with Acute Coronary Syndrome, so, it becomes important to repeat the ECG at regular intervals in such cases. Repeating the ECG may reveal the diagnostic changes.
Angina Syndromes
Angina pectoris is a clinical syndrome pertaining to coronary artery disease which is caused due to myocardial ischaemia which is manifested by retrosternal chest pain. Depending on the severity of occlusion Angina can be classified into three types :-
1. Chronic stable angina
2. Chronic unstable angina
3. Prinzmetal angina
ECG manifestations of Chronic stable angina in coronary artery disease:-
- 50% have normal ECG
- STD and T wave inversion may be present at rest
- STD >1mm especially in leads V5 and V6 forms the basis of reporting a positive stress test
- T wave inversion may also be found during stress test
ST segment depression and T wave inversion
ECG manifestations of Chronic unstable angina in coronary artery disease:-
- 50% will have abnormal ECG
- T wave inversion with or without STD
- Pseudonormalisation of resting STD can also be seen
ECG manifestations of Prinzmetal angina in coronary artery disease:-
- ST segment elevation
- Tall, upright, widened and pointed T wave
- R wave amplitude inceases
- S wave amplitude decreases
- Transient conduction abnormalities like transient Left Axis Deviation, transient left or right bundle branch blocks
- Arrhythmias like ventricular ectopics , non sustained VT and transient heart blocks can also occur.
Myocardial Infarction (MI)
ECG, being simple, reliable and easily available is universally accepted tool for diagnosing and risk stratifying the Myocardial Infarction and other coronary artery disease.
In patients with ischaemic symptoms, one of the following abnormalities must be present for diagnosis of MI:-
- Development of New Pathological Q- Waves.
- Presence of ST segment elevation or Depression.
- New onset Left Bundle Branch Block.
The changes in ECG should be present in two contiguous leads.
Depending upon the abnormalities in ECG, MI is divided into two main types:-
- STEMI (ST segment elevation MI)
- NSTEMI(Non ST segment elevation MI)
ECG changes in STEMI
ST segment elevation indicates subepicardial ischaemia (coronary artery disease).
STEMI has three phases of evolution-
1. Hyper-acute phase :- It is recognised by following ECG changes-
- Tall, Symmetrical, Peaked and Widened T-waves
- Slope elevation of ST segment
- Increased amplitude of the R wave
- Increased ventricular activation time
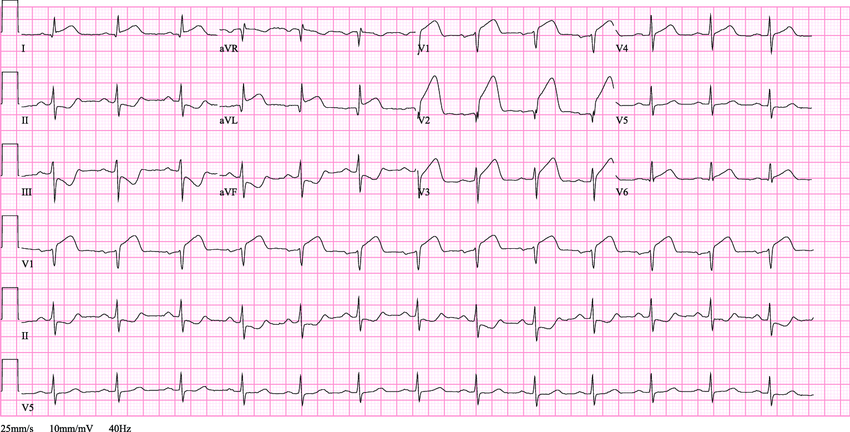
Hyperacute T waves of acute anterior MI – Tall, Symmetrical, Widened and Elevated T waves in V1 V2 and V3 .
2. Evolved phase :- It is recognised by following ECG changes-
- Appearance of new q waves
- Decreased R wave amplitude
- ST segment and J point elevation
- T wave inversion
- QRS broadening due to increased ventricular activation time
- QT prolongation due to increased depolarisation and repolarisation time.
Q waves, ST elevation and T wave inversion in evolved phase of STEMI
3. Chronic stabilised phase :-
- Q wave evolves maximally
- Elevated ST segment and J point returns to baseline
- T wave gradually regains positivity
- QT interval normalises
Localisation of the MI and culprit artery (in coronary artery disease)
1. Left Ventricular Myocardial Infarction
Left ventricle has three walls :-
- Anterior
- Inferior
- Posterior
Anterior wall is further divided into different areas like Antero-septal, Antero-apical, Antero-lateral etc.
The below table tells us the site of MI, coronaries affected and lead showing ST elevation.
Remember that there is reciprocal ST depression also which is not described in this table.
Anterior Wall MI
- STE in lead V1, V2 and V3
Posterior Wall MI
- Reciprocal STE in lead III and aVF
Inferior Wall MI
- STE in lead II , III and aVF
2. Right Ventricular Myocardial Infarction (RVMI)
Not very common but present in 30% cases of Inferior wall MI.
RVMI is more often related to arrhythmias than to pump failure.
ECG manifestations are as follows-
- STE in lead V1 or extra right precordial leads(V4r-V6R) of >/= 1mm.
- V4R being the most sensitive lead.
- Failure of reciprocal STD unlike AWMI so, this point is used to differentiate acute AWMI from RVMI.
3. Infarction of the Atria
Isolated infarction of atria is rarely recognised or reported because it is inconpicuous, small and difficult to evaluate and there is no distinctive clinical presentation.
ECG findings in atrial infarction
There is minimal elevation of PTa segment, in same direction as that of P wave
Sometimes there may be horizontal depression of PTa segment
P wave may become widened, slurred and notched
Atrial arrhythmias like Atrial Tachycardia, Atrial extrasystoles, Atrial fluter and Atrial fibrillation may be seen.
ECG changes in NSTEMI coronary artery disease
When ischaemia of sub-endocardial region occurs, there is STD instead of STE and the resultant entity is named as NSTEMI. NSTEMI may evolve into STEMI , so it is treated aggressively like that of STEMI.
ECG diagnosis of NSTEMI :-
- ST segment depression in precordial leads and lead I and II
- T wave inversion in precordial leads and lead I and II
STD in leads II, III and precordial leads V3 V4 V5
Arrhythmias in MI in coronary artery disease
1. Sinus Tachycardia
2. Ventricular Arrhythmias
Ventricular arrhythmias are most common cause of sudden cardiac death in a patient with MI.
- Ventricular ectopics
- Idioventricular rhythm
- Polymorphic VT
- Ventricular fibrillation
3. Atrial Arrhythmias
- Atrial ectopics
- Atrial tachycardia
- Atrial fibrillation
4. Sinus Bradycardia
5. Conduction blocks and heart block
- New onset LBBB (a criterion for diagnosis of acute MI)
- qRBBB
- Complete AV block in IWMI
- Second degree Mobitz II heart block occurs in AWMI due to IVS infarction
Diagnosing MI with LBBB
Diagnosing acute MI with previous LBBB
New onset LBBB is common in acute MI but diagnosing old LBBB in acute AWMI is a challenge because Old LBBB will mask the manifestations of acute AWMI.
This problem was solved by Sgarbossa et al by giving us criteria for diagnosing acute AWMI with old LBBB and is as follows :-
- Concordant STE of >1mm in atleast one lead (5 points)
- Concordant STD of >1mm in leads V1 – V3 (3 points)
- Discordant STE of >5mm in atleast one lead (2 points)
A total of 3 or more points is suggestive of acute MI in presence of previous LBBB without the need of further investigations.
Diagnosing Old AWMI with LBBB
- Cabrera’s sign – Notching in ascending Limb of S wave in leads V3 – V5
- Chapman’s sign – Notching in the upstroke of R wave in leads I, aVL or V6
- Presence of q waves in leads V5, V6, I, aVL is suggestive of old MI
That was all about ECG in coronary artery disease. I hope you have learned something meaningful in this article.
What chatGPT says about Coronary Artery Disease ECG?
Coronary artery disease (CAD) is a condition where the blood vessels that supply oxygen and nutrients to the heart muscle become narrowed or blocked due to the buildup of plaque (atherosclerosis). This narrowing or blockage can restrict blood flow to the heart muscle, leading to chest pain (angina), heart attack (myocardial infarction), or other serious complications.
Electrocardiogram (ECG) is a test that records the electrical activity of the heart. In in coronary artery disease, the ECG may show several characteristic changes depending on the severity and extent of the disease:
- ST-segment depression: This is a common finding in in coronary artery disease, indicating myocardial ischemia (lack of oxygen to the heart muscle). Ischemia in coronary artery disease occurs when blood flow to the heart is reduced due to narrowed coronary arteries.
- T-wave inversion: Inverted T-waves can be seen in leads corresponding to the area of the heart that is not receiving enough oxygen due to coronary artery narrowing or blockage. This is often seen in ischemic conditions like in coronary artery disease.
- ST-segment elevation: While this is more characteristic of acute myocardial infarction (heart attack), it can also be present in in coronary artery disease, especially during episodes of unstable angina or when there is complete blockage of a coronary artery.
- Abnormal Q waves: Q waves may appear larger or deeper than normal due to previous myocardial infarction or significant damage to the heart muscle caused by in coronary artery disease.
- Arrhythmias: in coronary artery disease can predispose individuals to various arrhythmias (irregular heart rhythms), which may be evident on an ECG.
These ECG changes can help healthcare providers diagnose in coronary artery disease and assess its severity. However, it’s important to note that ECG findings alone are not sufficient for a definitive diagnosis of in coronary artery disease; additional tests such as stress tests, cardiac catheterization, or coronary angiography may be needed for confirmation.
It is indeed a beautiful answer given by chatGPT for coronary artery disese ECG. AI has come a long way in medical field also.