
RBBB is a delay or block of conduction within the right bundle branch. In complete RBBB, the duration of QRS is >120ms and in incomplete RBBB it is between 100 and 120ms.
COMPLETE RBBB
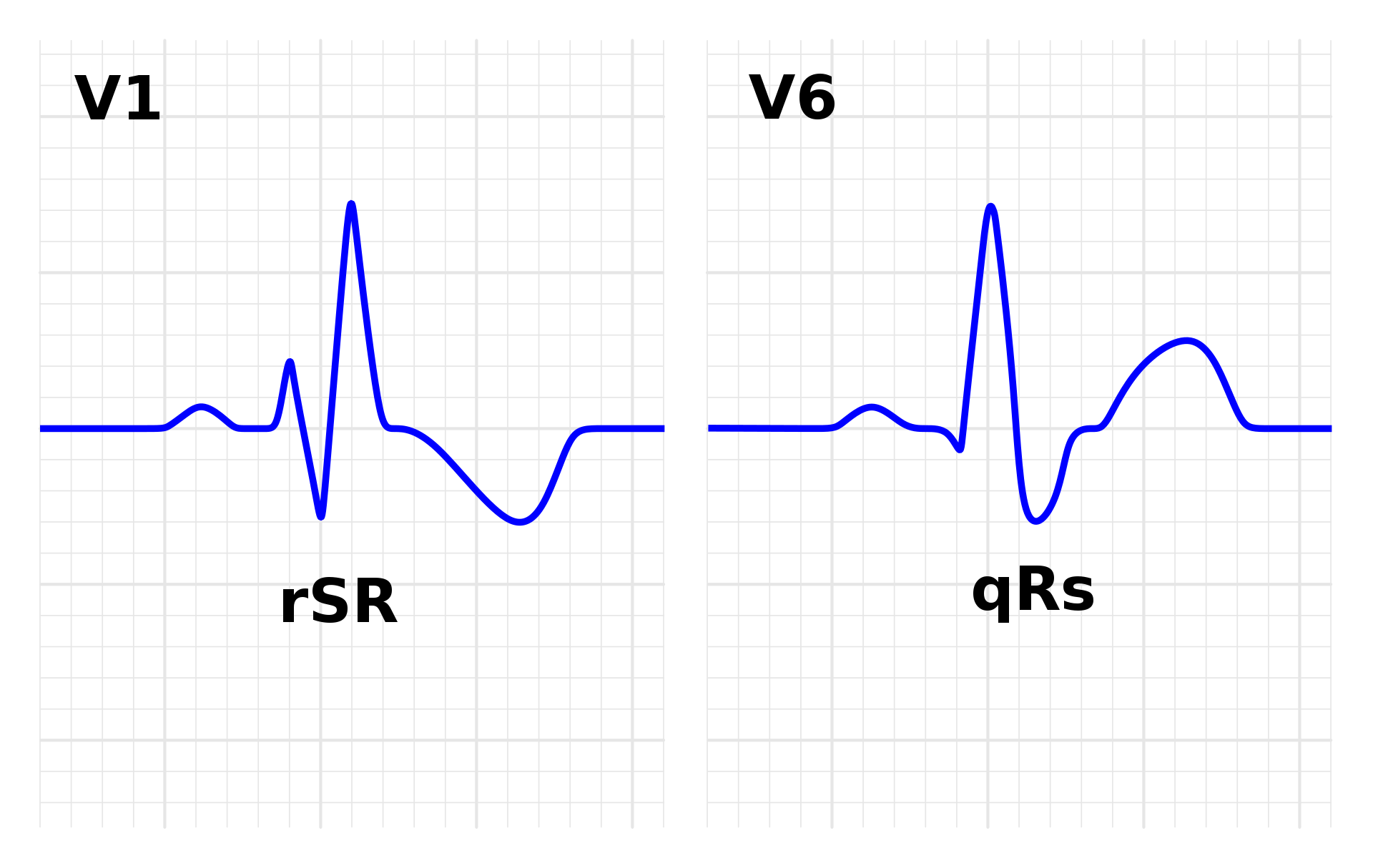
Criteria for RBBB
- QRS duration >120ms
- rsR pattern in lead VI with R’ >r
- Slurred S wave in lead I and V6
ECG manifestations of complete RBBB:
Leads orientated to the right ventricle, for example, lead VI, reflect the following:
- There is an initial small r wave due to left septal depolarization.
- This is followed by an S, or more likely an s, wave which is due mainly to depolarization of the left free wall. This S wave is attenuated and may even disappear completely.
- There is a terminal bizarre and slurred R wave (R’) due to late and anomalous right septal and right free wall depolarization.
Leads orientated to the left ventricle, leads V5 and V6, and standard lead I, reflect the following:
- There is a small initial q wave, due to left septal depolarization.
- There is a relatively tall R wave, due mainly to depolarization of the left free wall.
- There is a terminal bizarre and slurred S wave due to late and anomalous right septal and right free wall activation.
Mechanism
With complete RBBB, as with normal intraventricular conduction, activation of the ventricles begins in the left lower third of the interventricular septum and spreads transversely from left to right through the septum.
This left-to-right vector, however, is now no longer opposed by the normal smaller right-to-left septal vector that originates from the right bundle branch, and the right side of the interventricular septum.
And, since the left-to-right septal vector is no longer opposed, it is therefore minimally increased in magnitude.
This may result in a slightly more prominent initial r wave in lead V2 and it is this lead that is most aligned with this vector.
Normal left paraseptal activation occurs next, spreading transversely from endocardial to epicardial surfaces. This is followed by endocardial—epicardial activation of the free wall of the left ventricle. This free wall left ventricular vector is directed to the left.
Activation of the right side of the interventricular septum, and the right and free wall is effected by the activation front which arises in the left side of the interventricular septum.
This crosses — so to speak ‘jumps’ — a physiological intraseptal barrier and is then conducted through ordinary myocardial tissue, and not specialized conducting tissue, within the right ventricular wall.
This right-sided activation is consequently slow and anomalous in character, tending to be longitudinal or tangential rather than transverse (endocardial — epicardial).
The Purkinje system is programmed for the rapid transmission of the activation process from a central distributing point which is normally in the subendocardium.
Activation entering the system from another direction, that is within the myocardium, is also transmitted but in a bizarre, relatively slow and ineffective manner.
This results in slow abnormal depolarization of the right side of the interventricular septum, the right paraseptal region and the free wall of the right ventricle.
This slow abnormal depolarization is reflected electrocardiographically by large, slowly inscribed vectors which are directed anteriorly and to the right.
The abnormal right paraseptal vector 3 occurs simultaneously with, but is opposite in direction to, the vector of left free wall — vector 2.
These vectors thus oppose and therefore tend to neutralize each other.
This results in a marked diminution of the S wave in lead VI that in advanced degrees of RBBB or complete RBBB, may disappear completely.
This process also results in attenuation of the R wave in left-orientated leads such as lead V6. Unlike the effect on lead VI, however, the R wave in lead V6, while attenuated, is not abolished completely.
This is because lead V6 is orientated to the lower free wall of the left ventricle and, is thus influenced to a degree by the left paraseptal vector, which also contributes towards the positivity of the R wave in lead V6.
Right paraseptal activation is followed by abnormal and slow activation of the right free wall. This result in a large unopposed vector directed anteriorly and to the right.
It will be reflected by a wide R’ deflection in lead VI and a prominent, slurred and delayed S wave in lead V6.
The slow, abnormal, anomaIous form of activation is also responsible for the marked notching and slurring of the terminal bizarre and widened deflection.
Incomplete RBBB
The type of electrocardiographic manifestation which occurs in incomplete RBBB will depend upon the degree of delay within the rig ht bundle branch. Progressively increasing delay of conduction within the right bundle branch will result in a progressive sequence of electrocardiographic manifestations. These are considered below with reference to the right-orientated leads — leads VI and V2, especially lead V2.
Electrocardiographic manifestations of incomplete RBBB:
With progressive increase of delay within the right bundle branch, the following electrocardiographic sequence of progressively increasing incomplete RBBB manifests:
- There is This is the earliest sign of incomplete RBBB
- The diminution of the S wave is followed by slurring of the u stroke of the S wave in lead V2. This is usually associated with further diminution of the S wave.
- A small r’ deflection then appears in lead V2. This will result in an rsr’ configuration. The diminutive r’ is not widened and, is usually associated with further attenuatjon of the S wave.
- The amplitude of the R’ deflection in lead V2 then increases. This is a more marked manifestation of that described above. The S wave is further diminished, and the configuration is that of an rsR’ complex. While the QRS complex reflects a slight increase in duration, it is not increased beyond 110ms. The R’ deflection itself is not widened beyond 40ms.
Mechanism
- In the case of incomplete RBBB, conduction through the right bundle branch is still possible but it is delayed.
- A small delay within the right bundle branch causes a delay in the inscription of the right paraseptal vector.
- As a result, this vector now occurs synchronously with the free wall forces.
- Since vector 3c is directed slightly opposite to vector 3b, it will diminish the magnitude of the resultant vector 3 that is responsible for the S wave in lead V2.
- A slight delay in conduction through the right bundle branch will thus cause a diminution of the S wave of lead V2. There should also be a diminution of the R wave in lead V6.
- While this can occur, the manifestation is not consistent.
- A possible reason for this lack of consistency is that lead V6 tends to be more obliquely orientated, that is towards the left paraseptal vector as well as the left wall vector.
- It will therefore also be influenced by the left paraseptal vector that will contribute to the amplitude of the R wave in this lead.
- As the delay within the right bundle branch increases, activation of the free wall of the right ventricle will be increasingly delayed.
- And, when the delay is of such degree that activation of the free wall of the right ventricle occurs after activation of the free wall of the left ventricle, an r’ deflection will appear in the right-orientated leads.
- This is because right free wall activation is then no longer completely opposed by left free wall activation.
- The r’ deflection will become increasingly taller as the delay increases since a larger part of the right free wall activation will occur after left free wall activation.
- The R’ deflection of maximal delay, however, is not widened beyond 40 ms.
- When the R’ deflection is widened to >40 ms, the block may be considered to be complete and conduction no longer occurs through the right bundle branch but through ordinary myocardial tissue as explained earlier.
The significance of the anatomical length of the right bundle branch:
It is becoming increasingly clear that slowed conduction is not the only cause of conduction delay in the genesis of incomplete RBBB. The length of the right bundle branch may also play a significant role.
The normal right bundle branch is about 40 mm in length.
The normal conduction velocity in the right bundle branch is 2 m/s.
Thus, for each centimetre increase in the length of the right bundle, the conduction time through the bundle will increase by 5 ms (from 20 to 25 ms).
If, for example, the length of the right bundle branch is increased by 4 cm— a not uncommon occurrence with chronic right ventricular dilatation — the conduction time within the right bundle branch will increase by 20 ms or 0.02 s (4*5 ms).
If, therefore, to begin with, uncomplicated intraventricular conduction results in a QRS duration of 0.09 s, a 4 cm increase in the length of the right bundle branch alone will increase the QRS duration to 0.11 s.
If, in addition, there is also a conduction delay due to diminished conduction velocity, the Increase would obviously be greater.
The anatomical factor is clearly of significance when there is dilatation of the right ventricle due to volume or diastolic overload that occurs characteristically with atrial septal defect, and also with such conditions as chronic cor pulmonale and tricuspid insufficiency.
It is thus evident that incomplete RBBB does not necessarily imply a block or diminished conduction velocity within the right bundle branch, but that a potential anatomical factor must also be considered.
It is that COMMENTS may manifest without an increase in duration of the ORS complex.
The condition may first manifest with a mere attenuation of the.
S wave in lead V2, possibly associated with a slurring of the upstroke of the S wave in lead V2.
Whereas the diagnosis of complete RBBB is dependent upon the morphology as well as the duration of the ORS complex, thc diagnosis of incomplete RBP,B is largely dcpcndcnt upon morphology alone.
The ST segment and T wave in right bundle branch block:
- In uncomplicated RBBB, the T wave and ST segment will reflect secondary changes that are secondary to the abnormal intraventricular conduction.
- The T wave is opposite in direction to the terminal QRS deflection.
- Thus, if the terminal deflection is an R’, as occurs, for example, in lead VI, the T wave will be inverted.
- The associated ST segrnent will be slightly convex-upwards and, at times, minimally depressed.
- If, on the other hand, the terminal deflection is an S wave, as occurs, for example, in lead V6, the T wave will be upright.
- The associated ST segment will be slightly concave-upwards, and, at times, minimally elevated.
- Any deviation from these manifestations usually represents a primary change that is a primary myocardial abnormality in addition to the RBBB.
The significance of RBBB:
RBBB may occur in the absence of heart disease.
It has been reported in normal Air Force personnel with an incidence of 1.5 per thousand between the ages of 20 and 40 years, and 2.9 per thousand in individuals over the age of 40 years.
It may also be associated with coronary artery disease, various cardiomyopathies, Ebstein’s anomaly (in an atypical presentation), atrial septal defect and persistent atrioventricularis communis.
It may be a manifestation of an acute pulmonary embolism, when it usually indicates a massive embolus.
Consequently, RBBB must always be evaluated in the perspective of the associated clinical and electrocardiographic manifestations.
“In anterior infarction, develo ment of RBBB indicates proximal coronary artery lesion and has a worse outcome.
Clinical implications:
- RBBB can be seen as a normal finding in the absence of heart
- In the presence of heart disease, prognosis is related to the severity of the underlying heart disease.
- RBBB complicating acute myocardial infarction has poor prognosis.